6. Shmuel Harofe: difficulties and struggle
Upon our return to Israel we needed, first of all, a place to live. The hospital administration took care of this problem ahead of time and, on the day we arrived, we received keys to one of the houses kept by the administration for hospital employees. It was a modest two-bedroom wooden house (“Swedish barrack”), adequate as temporary living quarters for an unassuming family trying to take root in a new place. We could catch our breaths and start looking for permanent housing. We soon found and purchased one “on paper”: at the time of signing the contract, an old house stood on that site, ready for demolition. However, the contractor assured us that the construction of the new building would take no longer than two years. Indeed, in September 1973, just prior to the outbreak of the Yom Kippur War, we entered our own new apartment in Rehovot.
The immediate proximity of our temporary house to the hospital was very convenient, particularly during the first three years of my work, when I used to spend whole days in the hospital, from the early morning hours (before 7 o’clock) until after the evening bedside rounds, weekends included, and quite frequently nights as well. This exhausting schedule was the result of my early relationship with the two surgeons on my team. They viewed the appointment of an outsider as chief of the department, as an encroachment upon their ”rights”, sanctified by their longer presence on the service and their age. For them, I was an intruder without seniority, who had seized the position on the top of the pyramide and pushed them down.
As chief, I wanted to be in full control of the department. This was not only my right, but indeed, my obligation. In order to achieve this, I had to be present on the ward at all times. I had to write and personally sign every order; without it, none would be carried out. My work would be sabotaged – I knew this for sure. 13
The only person on the surgical service I could rely upon, was the head nurse, Nurit Firt. Nurit was a charming and hard-working woman, full of enthusiasm and initiative. She did not spare time and effort to save the service from collapsing. During the following years, my relations with my deputy, Dr. Shmuel Winter, improved markedly. We learned to work together, with respect for each other. Dr. Winter told me, repeatedly, that only since I came to Shmuel Harofe Hospital, did he start performing lung operations by himself. Under Dr. Herman, his participation in the operations was limited to opening and closing the chest. Dr. Winter remained my deputy until his retirement in 1980.
The second surgeon was quite a different matter. I despised him, and for obvious reasons, do not wish to reveal his name. Of course, my opinion might not be considered objective, but save for my own impression, I have no other sources to draw upon. In my appraisal, he was extremely lazy, incredibly stubborn and dishonest. On many occasions I discovered complications – the result of his negligent work, that he had tried to hide from me.
The following incident may serve as an example of his dishonesty. A patient who had undergone resection of the pilonidal sinus (abscess over the tail bone) came to me and complained that his operative wound failed to heal. Upon investigation, I found that this surgeon had operated on him, and at the end of the operation, had left a drain in the wound. At the time of closing the wound, the drain had been unintentionally caught in one of the sutures. When the time came to remove it, the surgeon pulled it forcefully, tearing the drain, so that part of it remained in the wound. The surgeon knew well that the wound would never heal as long as the foreign body remains inside, but he told the patient that the treatment has been successfully completed, and discharged him. The wound continued to discharge pus for many weeks, and the patient returned to the hospital. Upon opening the wound, I found the torn drain inside. I showed this to the surgeon. He smiled and said “I thought that it would heal”. I barely restrained myself from slapping his face.
His stubbornness and laziness are well exemplified by his refusal to take emergency night calls because of… his age. He was 51 at the time, and many physicians, his age and older, took night calls according to the needs of their respective services. Following his refusal, he simply ignored the rules and did not stay in the hospital while on a night duty. What could I do? I had no means to impose the law upon him, because of his tenure – a sacred and untouchable right in the Israeli labor relations. I could not fire him. In order not to leave the service overnight without a surgeon on duty, I had to stay in the hospital myself, or to look for surgeons from other departments (urology, orthopedics), or even from outside the hospital. Those surgeons would be strangers, who did not know the patients on the service at all. But nothing else could be done about it. I could only hope, pray, and wait for a miracle to happen. I do not usually believe in miracles, but perhaps this case should provide an opportunity to reassess my beliefs, because a miracle did, indeed, happen.
One day this surgeon told me that he needed two or three months leave of absence. A relative of his had died and he must go to France to receive a great inheritance. In view of the extreme shortage of doctors on my team, it was very inconvenient for me to let him go. But together with the hospital director, we came to a conclusion that we had no choice. The surgeon had accumulated a sufficient number of unused vacation days, and had a good reason to take them now. I had to consent to his request.
The leave of absence declared to last two months, started in February 1974. In May 1974 I received a letter from the surgeon. The return address was that of an attorney’s office in France. The Doctor asked for an extension of his leave for an additional three months, in order to “complete his business”. After another consultation with the hospital director, I granted him this extension too, but added that this one was final. If he does not return by the end of the additional three months, we would replace him. Following this, I did not hear from him for over a year. I wrote him several letters, mailed them all to the attorney’s office in France, but they remained unanswered. During that time, people who knew him well, told me that the story about the inheritance in France was a pure fiction; the surgeon was in Germany, where he tried to obtain a medical licence and find a job. The chances of his return to Israel were nil.
In November 1974, a doctor with a Russian accent asked for an appointment with me. Dr. Moritz Kaufman, a new immigrant from the Soviet Union, one year in Israel, was a general surgeon with 20 years of professional experience. During the past year he had worked in the Ichilov Hospital in Tel Aviv on a temporary job, but at the end of the year, no position could be found for him, and he was looking for work. I accepted him for a trial period. He came full of energy. It was the first time since I came to Shmuel Harofe, that I had in my department a surgeon with a positive approach, willing to work. He had experience, common sense and good clinical judgement, and always worked hard. He was a general surgeon, but while working with me, learned thoracic surgery as well. We became good friends. When Dr. Winter retired, he became my deputy. On several occasions he told me: “In 1974, when you set our appointment for 6 a.m., I thought that it was an isolated incident”. But he became used to the unusual working hours on my service. Until this day I do not understand why they had not kept him on at the Ichilov Hospital. It was, undoubtedly, their mistake, from which I benefited for the next 21 years. At the end of this period we both retired. 14
The surgeon who tried to settle in Germany, returned to Israel in 1975 and appeared before me without any announcement. He entered my room, the usual smile on his face, and said “I am back”. To this I answered “I am very happy to see you, but I wrote you several times that if you do not return by the specified date, we will be forced to look for a replacement. We found one. The position, previously yours, is now occupied by Dr. Kaufman.” “This position belongs to me. I have tenure. Kaufman can look for a job elsewhere”, answered the surgeon, this time without a smile, and left the room. Since then I have not seen him. Not seen, but I heard a lot. The struggle for the position in question lasted a whole year. It involved the Israel Medical Association and the Organization of Government Physicians, both of which supported the surgeon’s claim of his “rights”, but it also involved the executive director of the Ministry of Health, whose primary concern was the benefit of the very problematic Shmuel Harofe Hospital. The hospital had to be upgraded. It was a war in which I invested great efforts, letters, and innumerable hours of emotional argumentation at discussions devoted to this problem. Tenure is holy and untouchable… but at the end I won. Does anyone still doubt that miracles do happen?
When I started my job in Shmuel Harofe, I found there one more surgeon, who was not there during my “acquaintance” visit in December. Because of the severe shortage of staff, the hospital director looked desperately for a surgeon, and found an unemployed one. He appointed him to the surgical staff, in spite of the fact that during the preceding two years the new surgeon had been appointed on a trial basis in 12 different departments of surgery in virtually every hospital in Israel and was fired from each one promptly. It did not take me much time to discover that he was a difficult psychopath and an incurable liar. Fortunately, he did not have the “holy” tenure, so I promptly initiated the proceedings for dismissing him. He reacted to the letter of dismissal by beating up the hospital director and wrote to the Ministry of Health malicious letters of accusation against me, the hospital director and the hospital.
Getting rid of these two surgeons was a very important and decisive step in improving the status of my department. In parallel, I applied to the Scientific Council of the Israel Medical Association (the equivalent of the American Board of Medical Specialties) for accreditation to provide residency training to surgeons. A commission was appointed and the term for its investigation was set for April 1972. The moment I saw the three surgeons, members of the commission, entering my office, I knew that my chances of passing the test were nil. The Commission Chairman was that thoracic surgeon from the Rambam Hospital, involved in the old “Abouav affair”. He knew me, knew that I was Jack Abouav’s friend, and there was strong feeling of aversion between us. The second member of the commission was Dr. Joseph Borman from Hadassah – a former student and friend of the chairman. That was enough. The third member was Dr. Dintsman from the Beilinson Hospital. He did not know me and had no incentive to struggle in my favor.
The “investigation” by the Chairman of the Commission was particularly traumatic. In striking contrast to the custom of such investigations (in later years I participated in them many times), he did not concentrate on the number of operations done on my service, nor on their variety; not on the function of the supporting services in the hospital, such as the Institute of Pathology, the Emergency Department and others, nor on the availability of other services (e.g. urology, orthopedics) on which the residents would spend part of their training (“rotation”). Instead, he chose to concentrate on the number of patients who died on my service after prolonged illnesses, digging from under the earth “complications” that supposedly could have been prevented, had we tried hard enough, and other similar allegations. The investigation was intentionally antagonistic and ended with the unavoidable and expected result: the accreditation was not granted.
In the beginning of 1973, less than a year since my failure with the first commission, I was granted a second chance. This time the composition of the committee was different and the investigation was conducted in an objective, unbiased spirit. In spite of the fact that no great changes could have occurred in the hospital and in the function of my department in such a short time, the members of the committee did not have any reservations and my department was granted full accreditation for training of surgeons. Many came; some were from other hospitals, interested to spend rotation on my service. The work became more interesting and academically oriented.
The residents were happy with their training and some asked for extension of their rotation period, which was usually granted. A rather striking example of such turn of events was Dr. David (Dudu) Schneider, a resident in gynecology and obstetrics at the Assaf Harofe Hospital. The curriculum of his residency included a six-months rotation period on a surgical service, and he chose to do it in my department. Close to the end of his rotation he asked Prof. E. Caspi, his chief in Assaf Harofe, to let him stay on my service for an additional period of six months. Professor Caspi consented. After that came another request for a six-months extension, and another one. Altogether, Dudu Schneider spent a full two years on my service. He was satisfied with the experience gained and won the highest appraisal of the entire staff. He was a charming fellow and an intelligent and industrious physician. During his rotation, besides the routine work, he managed to write two clinical papers, which we published together.
Medical students also came to my department, initially for their elective period of study – one or two months at a time. The first student who came was Richard Reznick from Canada. My friends, surgeons in Toronto told him about me, and he decided to spend his elective month on my service. We were “on the map”. Today Dick Reznick serves as Professor and Chairman of the Department of Surgery at the University of Toronto Faculty of Medicine. Training residents and teaching students demanded great efforts, in which the help of Dr. Kaufman was of inestimable value.
In the early 1970s only four hospitals in Israel had departments of thoracic surgery: Hadassah in Jerusalem, Rambam in Haifa, and two hospitals in the Tel Aviv area – Beilinson and Tel Hashomer. In addition, there was my department – thoracic mixed with general surgery. Because other hospitals did not have services of a thoracic surgeon, I was frequently called for consultations, and the patients were transferred to my department for operations. Particularly good relations evolved with three hospitals: Hadassah-Rokach in Tel Aviv (today part of the Sourasky Medical Center), Assaf Harofe and Kaplan. However, I was also frequently called to other hospitals. On several occasions I operated in the Meir Hospital in Kfar Saba.
Soon after entering my job in Shmuel Harofe, I started performing operations that were not done in Israel before. The first one was, quite naturally, mediastinoscopy – that exploration of the mediastinum, which I did in Mississippi in 1967. I was the first surgeon to perform it in Mississippi, and now, the first one in Israel. Since 1971, this procedure became routine in my department, before every resection of lung cancer, as part of the preoperative workup. Many patients were referred to me from other hospitals for this operation, before it became common.
Another operation, that according to my knowledge, no one performed in Israel before me, was the resection of the trachea, because of a tumor, or a scar with an obstruction. During the 1970s I performed more than 20 such operations in Shmuel Harofe, and several others on visits in Meir and Assaf Harofe Hospitals. It should be pointed out that all tracheal resections at Shmuel Harofe, were performed in patients referred from other hospitals.
Pleuroscopy 15 had been in clinical use in the first half of the twentieth century, mainly in the evaluation and treatment of tuberculosis. With the discovery of drugs against tuberculosis and the development of techniques of pulmonary resection, the importance of pleuroscopy declined markedly, and gradually its use was discontinued. The early 1970s brought renewal of this method, not in the management of tuberculosis, but for diagnostic purposes, mainly in patients with pathological changes in the chest cavity, such as masses or collections of liquid. In 1974, my department was the first one in Israel to reintroduce it into clinical use, and in 1980, at the convention devoted to pleuroscopy in Marseilles, France, I presented our early experience with this method in three lectures.
In general surgery, likewise, an invigoration occurred in my department. Patients with major problems in need of surgery, who until recently were referred from the Department of Medicine to other hospitals, started coming to our service. In 1971 and 1972 we did our first porta-caval shunts 16 ─ the operation that Dr. Erlik was doing in the 1950s as a pioneer, and which I observed him perform when I came for my interview; radical neck dissections for cancer of the neck; resections for cancer of the esophagus with transposition of the stomach into the chest; fundoplication 17 ─ at that time a new operation in Israel; and others. Most of these operations were done in Israel before, but never in Shmuel Harofe Hospital.
At that time I was still interested in surgery of blood vessels, and I performed such operations from time to time. However, for good practice of this branch of surgery, one needs special instruments and a unique installation for angiography. 18 We did not have all these, not even the special needle needed to inject the contrast medium. I received one such needle, a used one, from Prof. Pajewski, chief of the Radiology Institute at Assaf Harofe Hospital. I used it several times successfully, but this was not enough. I talked about it with my former chief, Prof. Erlik, and with Prof. Mark Mozes from Tel Hashomer, both pioneers and leading vascular surgeons in Israel. They managed to convince me that one cannot practice vascular surgery in the 1970s, using methods and equipment of the 1950s. Complications are likely to occur. Furthermore, Prof. Erlik told me: “You cannot be a successful specialist in all three branches: thoracic surgery, general surgery and vascular surgery. Each one demands time for itself. Leave something to others…” Rather than waiting for complications, I decided to follow his good advice and gave up on vascular surgery.
I continued doing only one kind of operation classified as “vascular”, but in which no procedure is performed directly on the blood vessels. There is a condition of excessive palm sweating (hyperhidrosis), caused by a disproportionate function of the autonomous (sympathetic) nervous system. Excision of a short segment of the sympathetic nerve (the segment that affects the palm sweating) brings sweating back to its normal level. This operation is not new. It was conceived and carried out for the first time in 1949 by my old teacher in New York, Dr. Robert Goetz, while he was working in South Africa, before moving to the United States. 19 This operation is not difficult, trauma to the patient is minimal (a 5 cm. incision in the armpit) and the results are excellent. There is no need for any special instruments or radiograms, and every surgeon acquainted with anatomy of the chest and with the physiologic basis of the operation, can perform it. I learned it from Dr. Goetz, while working in his laboratory in New York. In Shmuel Harofe, I introduced this procedure into routine use, and patients started arriving in impressive numbers. Nowadays, this operation is performed in many hospitals in Israel, and the technique for its execution has changed somewhat.
* * *
The building of our apartment house lasted two years, and in mid-September 1973 we moved to Rehovot. Of course, we had no telephone. In the 1970s, waiting for a telephone line in Israel (for someone without connections) could last up to 10 years and more (yes, ten years, no mistake), and cellular phones were not yet invented. I hoped, that due to my function as chief of surgery in a government hospital, my waiting period would be shortened, but at the moment we did not have a phone connection.
On Yom Kippur day, October 6th, we were all at home. As usual on that day, there were no radio broadcasts; in fact, we were effectively isolated from the world. Should I suddenly be needed in the hospital for any reason, they would send an ambulance to bring me. There was quiet and tranquility and I was reading a book. A knock on the door interrupted my rest. Our neighbor, a military reserve paramedic was suddenly called to service. Military maneuvers on Yom Kippur? We turned the radio on and the broadcast was on. This was the way we found out that the war had started.
I went to the hospital. The hospital director and his deputy were already there, as well as a group of military officers from the Medical Corps. Within a short time, most of the physicians and the other senior employees were in the hospital. Dr. Davidson explained the situation. All wounded prisoners of war would be concentrated in one hospital, and Shmuel Harofe was selected to be the one. We had to quickly organize to be ready for an influx of wounded prisoners. The plan included:
- Maximizing the number of available beds. This would be achieved by discharging nearly all of our current patients. Those who could not be discharged, would be transferred to other hospitals.
- Converting as many barracks as possible into “surgical” units.
- Organizing the work of all physicians in the hospital, and adjusting it to the conditions of war.
- Preparing a daily working schedule with detailed hours, and a list of emergency calls.
- Organizing the Emergency Department.
- Organizing the Operating Rooms.
- Preparing a helicopter landing pad.
With regard to Point 1, discharging patients and freeing beds – most of our patients could be discharged either immediately or within a couple of days. Transferring patients to other hospitals was impractical, as all the other hospitals were also preparing for the war and needed free beds. None would accept civilians from Shmuel Harofe. Thus the patients who could not be discharged, were concentrated in one barrack, and were taken care of by their respective physicians.
Point 2 did not present any special problems – the necessary equipment for wound care and change of dressings was brought from the storerooms.
Point 3, organizing work of the physicians, meant concentrating the greatest efforts on treatment of the wounded. Teams were formed, composed of doctors with different expertise (internists, pulmonologists, etc), with one surgeon (from any surgical subspecialty) for every team.
The new daily working schedule was identical for all the medical and surgical staff: 36 hours of work, followed by 12 hours of rest. The 36-hour working period started in the morning and ended in the evening of the following day, when the physician would leave the hospital for the night. This way, we were all in the hospital during the day, every day, while half of us stayed in the hospital for the night. This was not entirely my own original idea. I followed the example of my residency at the Albert Einstein – Bronx Municipal Hospital Center.
The Emergency Department and the Operating Rooms were staffed by surgeons, urologists and orthopedists, who used maximum flexibility and adaptation according to the volume of work.
Point 7 was, of course, not my concern. The helipad was prepared by an Army team.
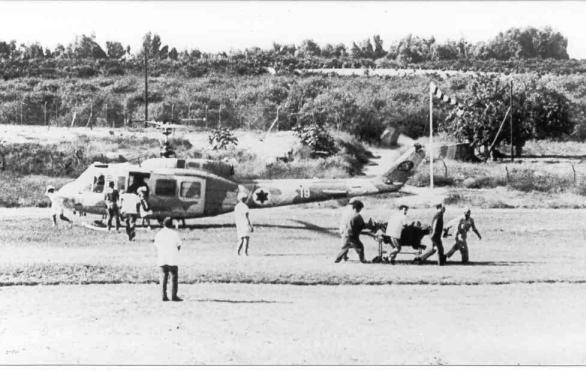
The wounded were brought by ambulances or by helicopters, usually in groups (Fig. 46). There were hours of relative quiet, but when a wave of 20 or 30 casualties hit the emergency room, all changed in a moment, and the team worked under pressure. In every group of wounded there were some severely injured and some who needed operations. The shortage of working hands was overcome by an excellent cooperation between the Emergency and the Operating Room teams. In addition, when needed, groups of “internists” were temporarily transferred from the “wards” (barracks) to the Emergency Department. Classifying the wounded and making early decisions demanded particularly great responsibility, often more than that required by the operations, therefore, the senior surgeons, those with the greatest experience, spent most of their time in the Emergency Department.
The small staff of Shmuel Harofe Hospital could not handle all these demands by itself. We needed enforcements. Many Jewish physicians, among them experienced surgeons from various countries, felt a need to contribute to the war effort. They interrupted their usual occupations and volunteered to work in Israel. Upon their arrival, they were distributed to various hospitals; some were sent to Shmuel Harofe. Their work was of inestimable value, and I will never forget them. Dr. Ashkenazy, an Israeli, interrupted his surgical residency in Buffalo, U.S.A., and worked in Shmuel Harofe. Professor Gurevitch arrived from Britain and contributed from his extensive experience. Dr. Alan Gross arrived from Canada. I had met him several years earlier, during my fellowship at the University of Toronto, while he was a resident in orthopedics. He came to Israel full of enthusiasm and worked hard until the end of the war. Later, he was promoted to the rank of Professor and Chief of the Department of Orthopedics at the University of Toronto. Dr. Alan Padwell, a young physician, just beginning his training in surgery, arrived from Britain. After the war ended, he stayed in Israel and continued his surgical residency in my department. Eventually he married a charming English young lady and returned to Britain.
I developed a particularly warm relationship with a volunteer from Boston, Dr. Theodore (Ted) Waltuch. This young surgeon was certified both in general and in thoracic surgery. He worked with amazing industriousness beyond the “official” hours, under hard and primitive conditions, so utterly different from those he was used to in Boston. His enthusiastic approach to work and to helping the wounded was exemplary. After the war we remained friends and kept close contact. He returned to Israel for a visit, and during several of my trips to the United States, I visited his home, met his family and lectured at the staff meeting in his hospital. Last year Ted died from heart disease. Blessed be his memory.
To complete the picture, I cannot avoid mentioning another, less exemplary case. About a week into the war, a vascular surgeon from the United States came to Israel. Because of his expertise in vascular surgery, he was referred to Shmuel Harofe, as we did not have a good vascular surgeon. He did not hide his unhappiness with being referred to treat prisoners of war, and said: “I came to help Jews, not Arabs”. I replied that helping in our war effort certainly helps Jews, and a conscientious physician cannot abstain from treating wounded enemy soldiers. He seemingly agreed with me. Then I showed him our working schedule, pointed to his working hours and nights on call, and we agreed that he would enter his schedule the next morning. However, he did not come. Neither the next morning, nor evening. And not the following day. He did arrive at my office ten years later, with his new wife, before whom he praised himself and his heroic deeds as a war “volunteer”. I did not want to embarrass him in front of his wife, therefore I did not correct his chivalrous stories, but also I did not praise him for what he had not done ten years earlier.
During the war we admitted to the hospital 779 wounded soldiers. Of these, 284 (a little over one-third) were operated on. Ten prisoners died from their injuries. Seventy-seven wounded had penetrating chest injuries (10% of all). There were no deaths in this group. One particular point is worth stressing: although all chest wounds were contaminated and 70 of the 77 were grossly dirty, full of sand, clods of earth and torn clothes, only in one patient (1.3%) did an empyema (purulent infection in the chest) occur. Review of data from the Vietnam War disclosed a 6% empyema rate among the American soldiers with chest injuries. This big difference can probably be explained by the different background of the casualties. The majority of the Egyptian and Syrian combatants were from rural areas. In contrast to the urban Israeli population or to the U.S. combatants in Vietnam, they had rarely received antibiotic treatment in the past. Thus their microorganisms were not resistant to antibiotics, and the first antibiotic treatment gave immediate good results. This phenomenon was particularly striking among soldiers with chest injuries and those with burns. 20
The wounded remained in the hospital for a long time beyond that justified by their medical condition, because it was impossible to discharge them “home” or to a convalescent home. They had to stay, until they could be sent to a camp for prisoners of war, which usually meant some time after their complete recovery. Thus they continued to occupy valuable beds, keeping the hospital full to capacity, until the end of the war. A surplus of casualties, for whom no place was available (to the best of my memory, over 30 combatants) were hospitalized in the Assaf Harofe Hospital. Those in need of neurosurgical treatment, were hospitalized at the Sheba Medical Center in Tel Hashomer.
We developed good personal relations with some of the Egyptians, and from time to time we heard a few words of thanks. I remember a young military physician injured in the chest and with fractures in three of his limbs, all in a cast. We conversed almost every day and, as an expression of our special relations, gave him a separate room. In contrast to the Egyptians, we never heard a word of thanks from the Syrians; their eyes and conduct expressed only deep-rooted hatred, and they did not engage in any private conversations with us.
The cease-fire agreement with Egypt was signed in December 1973. Soon thereafter, most of the Egyptian prisoners were freed, and we returned to “civilian” surgery. The progress with Syria was slower and their prisoners remained with us until January 1974 (Fig. 47).

Fig. 47. The deliberations preceding discharge of prisoners; the hospital director, Dr. Davidson, first from right, in white coat.
On November 17th 1973, Nurit, the head nurse, left the service for maternity leave and the same day gave birth to a daughter. Another nurse took her place on the surgical service. At that time I thought that the replacement was temporary, but it was an illusion. As I later found out, the substitute nurse agreed to replace Nurit under the condition of permanency on the service. When Nurit returned from her leave, it was to a different service, not to surgery.
During the 1970s the Shmuel Harofe Hospital made great progress. Much had been achieved. However, at the same time there were serious considerations in the Ministry of Health, to convert the hospital into a geriatric institution. Finally, in 1979, it was announced that at the end of the fiscal year, Shmuel Harofe will be converted from a general to a geriatric hospital. No one knew what would happen to the acute services, such as surgery, that do not belong in a geriatric institution. Various ideas were discussed. One possibility was to merge Shmuel Harofe with the Assaf Harofe Hospital, located in close proximity, and transfer our acute services to Assaf Harofe. At the same time, the construction of another hospital had just been completed. This was the Wolfson Hospital in Holon, supposed to replace the old and obsolete Donolo Hospital in Jaffa. Toward the end of the year, stormy deliberations were repeatedly conducted in the Ministry of Health with regard to the future of the various departments at Shmuel Harofe and their personnel. I did not participate in these meetings and do not know many of the details. Some may have been left intentionally undisclosed. The entire affair was characterized by immense tension between the teams of the various departments. A strong feeling of deprivation developed among those supposed to remain at Shmuel Harofe. The final decision was that the departments of orthopedics, urology and medicine (Second Department), would be transferred to Assaf Harofe, while the first medical department, surgery and one of the pulmonary services with its respiratory intensive care unit – to Wolfson.
I remained in Shmuel Harofe until the end of the fiscal year – March 31st 1980, when the operating rooms and the Emergency Department were closed, and the acute departments were transferred, each one to its respective new place.
The 9-year period at Shmuel Harofe was very important for me. During that time two of my children were born: Limor Tal, in January 1974, while we were still under the shadow of the Yom Kippur War; and Avishai Moshe, in September 1975. Avishai was named in memory of our fathers: Milka’s and mine. 21 I learned to be independent and to direct a hospital department. I did commit some errors, but also had successes. And I played a significant part in putting Shmuel Harofe “on the map”. In my judgment, the conversion of Shmuel Harofe into a geriatric institution was a success. Today it is a magnificent geriatric hospital, in my opinion the best in Israel. We did have part in making it such by building the foundations. In spite of all the difficulties, it was a beautiful era.
13 For a non-Israeli reader I must clarify that in Israel, after one year of uninterrupted work, every government employee is automatically guaranteed tenure and cannot be fired, no matter how inadequate his work may be. Exceptions include major crimes, but never “minor” misdemeanors such as absenteeism, negligence, or any kind of inadequacy at work. My dissatisfaction with the two surgeons on my team could never have served as a reason for discontinuing their employment.
14 Dr. Kaufman died in April 2001 of incurable illness. A close friend, an excellent surgeon, and a gentleman.
15 Pleuroscopy – observation of the inside of the chest cavity through an instrument inserted between the ribs. This procedure enables performance of certain lung operations.
16 This operation lowers the blood pressure in vessels bringing blood from the intestines to the liver. It is indicated in patients who suffer major bleedings because of cirrhosis (a chronic liver disease).
17 Operation for prevention of the flow of gastric contents into the esophagus.
18 Roentgenography of blood vessels with simultaneous injection of contrast medium.
19 My work and personal relations with Dr. Goetz are described in Chapter 3.
20 D. Weissberg. Treatment of thoracic injuries. Annals of Thoracic Surgery 1986; 42: 348.
21 AVISHAI: Avi – in Hebrew “my father”; Sh – short for Shmuel, Milka’s father; I – short for Israel, my father. Moshe was the name of my late brother.