4. Mississippi
In applying for residency in thoracic surgery I took into account several considerations. I felt certain that I could get an appointment at the Albert Einstein. But this was not what I wanted. During each year of my residency I spent a month or two on rotation on the thoracic surgery service and I had already learned well the routine of the department. Now I was looking for a change: I wanted to meet different surgeons and learn different methods and approaches from them. I wanted to work in a department with a predominance of pulmonary rather than cardiac surgery. Furthermore, I thought that after five years in New York, it might be better to move elsewhere and spend time in a different part of the United States. Above all, I was interested in a department with a good training program, and a leader in surgical progress. With Dr. State’s recommendation I could apply to the best and most prestigious institutions, with a good chance of being accepted in one. Friends advised me to visit the hospitals where I applied and to get a personal impression of the places of my choice, before committing myself anywhere. I took that advice seriously and traveled to several medical centers for exploratory conversations with surgical residents. To my surprise, I discovered that the most prestigious hospitals were not necessarily the best ones for learning. After much hesitation, I applied to eight medical centers and was accepted in four. The hospital that suited my needs best was the University of Mississippi Medical Center in Jackson. It was not the most prestigious hospital on my list, but the Chairman of the Department, Dr. James Hardy was a known pioneer in surgery. Among his many accomplishments were the world’s first human lung transplantation (1963) and the first ape-to-man heart transplantation (1964). Dr. Hardy’s response to my letter was encouraging (Fig. 15). In March 1965 I met him during his visit.
in New York, in September 1965 my acceptance was formalized (Fig. 16) and in the last week of July 1966 I crammed all my possessions into my old battered Volkswagen beetle, and went on a one-way trip to Mississippi. On the way I took time to visit places of interest, among them the Shenandoah Valley, the Luray and the Skyline stalactite caverns in Virginia, the battlefields of Gettysburg and other historic sites from the Civil War. On the evening of June 29th I arrived in Jackson and stayed in a hotel. The next morning I went to the Medical Center and in one day of fervent activity, managed to meet all the secretaries of Dr. Hardy, register in the hospital offices and obtain a bachelor apartment in the Medical Center. Already on my first day in Jackson I encountered difficulties in understanding the English spoken in the South. It took me some time to get used to it, but today I hear and understand the southern drawl without difficulty.
* * *
Each year Dr. Hardy accepted one resident for two years of training in thoracic surgery. During the first year the resident occupied a junior position in relation to the second year thoracic resident, but he was senior in relation to the general surgical residents. This particular state of affairs existed because there was no administrative division between the thoracic and the general surgical services. All surgical patients in the University Hospital – general, thoracic and vascular – were hospitalized together, and were taken care of by one “house staff” – the team of surgical residents. This arrangement, which also existed in the Veterans Administration Hospital in Jackson, enabled the general surgical residents to become involved and gain experience in thoracic and in vascular surgery throughout their training. However, this arrangement also created tension between the general surgical and the thoracic residents, because we, the thoracic residents, were “taking” all the thoracic and some of the vascular cases, considered “best”, from the generalists.
The entire Medical Center included both these hospitals, as well as the School of Medicine and, in addition, the Mississippi State Sanatorium – a hospital for tuberculosis located in Magee, 75 km (45 miles) from Jackson. The head of this whole surgical empire was Dr. James Daniel Hardy.
In addition to routine clinical work, each resident participated in some kind of laboratory research project, and the further one advanced in clinical surgery, the stronger was the research obligation. I was involved in lung and heart transplantations in dogs. This work was done in the laboratory for experimental surgery, three to four hours a week, usually in the afternoon (Fig. 17).
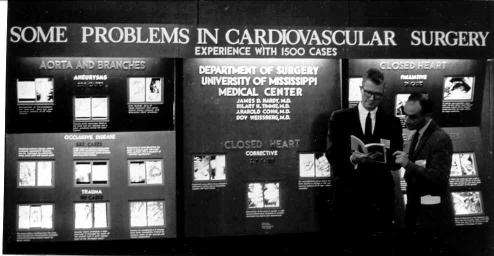
Fig. 17. With Dr. Hardy and our exhibit at the Convention of the American College of Surgeons, 1967.
The entire period of my stay in Mississippi was characterized by loneliness, especially if one considers the plentiful social life (within the possibilities of a surgeon-in-training) that I had in New York. The thoracic resident one year ahead of me was Dr. Suheil Saleh, an Arab born in Palestine. In 1948 his family moved to Jordan, and he studied medicine in Beirut. We never worked together: when I was at the University Hospital, he worked at the Sanatorium; due to rotation between the three hospitals we were separated most of the time. This way political frictions were avoided, except for a short-lasting increase in tension during the Six-Day-War.
There were about 150 Jewish families in Jackson and around 100 families more in the remainder of the State of Mississippi. But the main problem was not just the small number of Jews in the area. In the past, in my youth in Poland and later in New York, I had quite a few non-Jewish friends, and I felt well in their company. But I did not find a common language with the Mississippi gentiles. Their way of life was utterly different from mine. They never understood my background and my past, and I never showed any interest in hunting, fishing or football (American or European). I like photography, opera, history books... There is no doubt in my mind that there were people like me in the southern states, but I did not have an opportunity to meet them. Many of my gentile acquaintances in Mississippi tried hard to be friendly with me, but usually the conversation centered on their attempts to educate me about Jesus and to point out (for my benefit, of course) my erroneous ways without him. Still, for whatever reasons, I was not in want of Jesus. In spite of many invitations, I had no desire to attend religious ceremonies in churches and listen to sermons, interesting and eye-opening as they may have been. So I remained lonely.
Nevertheless, I found a way to the Jewish community. Before I left New York, my old friend, Dr. Ronald Dee (the chief resident in the beginning of my training), provided me with the telephone number of his relatives in Jackson. They invited me to their home, and later to the temple on Friday night. All the Jews, even those from distant towns where only one Jewish family lived (there were several such towns) used to attend services on the Sabbath. They, like me, missed the company of other Jews, and every Friday night, the only temple in Jackson (reform) was full to capacity. This way I became acquainted with the entire Jewish community in the State of Mississippi. It was the first time in my life that I have been to a reform temple. The rabbi and the majority of congregation prayed with their heads uncovered, although there was no penalty for wearing a skullcap. Some people covered their heads. Men and women sat together. In general, this institution called the Jewish Temple reminded me more of a Christian (Protestant) church than a synagogue. Is this important? I do not know. But the entire show, when seen for the first time, seemed strange. Still, I believe that it was better to attend this “unusual” synagogue, than to remain completely separated from the Jewish community. They welcomed me with friendliness and hospitality. A lonely Israeli, the only one in their town and in the entire state, stimulated the interest and curiosity of many. There was a local chapter of Hadassah Organization, and here, at their court, was a young physician, a graduate of Hadassah, “made in Israel”. Several families invited me to their homes, usually for dinner, but also for a lecture: they wanted me to tell them about Hadassah. I had plenty of relevant slides, and used them in Jackson as best I could.
The approach to work was most serious. Dr. Hardy insisted on it and gave a good example. He made bedside rounds every day, including Sundays. All physicians, from the most senior ones to the most junior interns, and all medical students had to participate. On Sundays the rounds had to be over by 11 a.m., so that people could go to church, therefore it started early in the morning. Dr. Hardy burst with energy and was short on patience. He never waited for an elevator. After completing the rounds on the first floor (adult service), the entire retinue leaped upstairs to the pediatric surgical service on the seventh floor. No one would wait for the elevator, while the boss practically ran up the stairs.
Heart operations were scheduled two days a week. After a heart operation, the resident who participated in the procedure (in essence, always myself), stayed with the patient without a break until the next morning. I used to sit next to the patient’s bed in the Intensive Care Unit all through the night, and if there was anything to do for him, I did it. In the free time I memorized all available current information on the patient, including the results of the most recent laboratory tests (tension of blood gases etc), in order to have instant answers ready for the chief’s visit. He usually came late at night or just before dawn, asked questions and gave example of devotion to the patient and profound knowledge of his problems. However, despite the efforts, the results of our heart operations were not satisfactory, and I did not find much interest in them. I studied cardiac surgery, because this was part of the material I needed to know toward the board examinations, but at this time I was already determined not to continue with it after the completion of my residency. In contrast, the pulmonary and vascular surgery results were exemplary. The team of surgeons included several who accumulated extensive experience in this field and were excellent teachers.
I learned, made progress, and the day was approaching when I would perform my first pulmonary lobectomy. The operation was planned for September 24th that coincided with Yom Kippur. I asked Dr. Gus Neely, the senior thoracic surgeon on the case, to postpone the operation for a day or two. I tried to explain to him what Yom Kippur was and why it was important for me not to operate on that day. But Dr. Neely was not agreeable, and my reasoning did not impress him. He thought that because of my laziness I simply did not want to work on a holiday. He issued a verdict that the operation will be performed as scheduled, with or without my participation. He knew that not performing the lobectomy would be a punishment for me, and was fully satisfied with it. Other residents did not understand my problem. Some asked: “Why can’t you just operate and then go on to celebrate?” For non-Jews in Mississippi it was totally impossible to grasp the meaning of Yom Kippur. Holidays are for celebrating, not for mourning and fasting. I stopped explaining, and on Yom Kippur did not come to work at all. Instead, I went to temple and stayed there – for the first time in my life – the whole day. The operation was performed by another surgeon. Dr. Hardy knew about the incident, but did not interfere. And I was left with the feeling that I did the right thing. It gave me more satisfaction than the lobectomy would have.
The best part of my work was the rotation at the Sanatorium in Magee. This 250-bed hospital was for patients with advanced tuberculosis, coming from the entire State of Mississippi. The work was done by a team of pulmonary physicians. The only surgeon in the house was the thoracic resident from the University Hospital – myself during the six months of my rotation. Three times a week one of the senior thoracic surgeons from the Medical Center in Jackson used to come to the Sanatorium to teach and help me with the operations. The majority of operations were in patients with pulmonary tuberculosis, but there were also many with lung cancer, infectious diseases of the lung and chest cavity, lung cysts, emphysematous bullae and other problems. I also did all the surgical work outside of the chest. For operations on gallbladder, uterus or prostate I contacted the appropriate expert at the University Hospital and made an appointment for the operation date. I performed all the operations, with the experts’ help.
Three senior surgeons instructed me on lung operations. The most prominent character was Dr. Gus Neely - the one who refused to yield on that famous “Yom Kippur lobectomy”. In the much smaller community of the Sanatorium, without disturbances from the “audience”, Dr. Neely learned to appreciate my work, and the relations between us improved greatly. We remained friends until my last day in Mississippi. I know that his reports to Dr. Hardy on my performance as resident were excellent. The second surgeon, Dr. Jesse Wofford, could be best characterized by his extreme religiousness. He served as a part-time Methodist preacher. On every occasion (suitable and unsuitable) he used to bring up the subject of Christian faith and ask me what I think about Jesus. My usual response that I do not think about Jesus did not satisfy him. Apparently he saw the opportunity to convert me to Christianity as his most important human obligation. It seemed obvious to me that his efforts will not stop as long I remain in Mississippi. In fact, he did not stop even for years after I left. I happened to meet Dr. Wofford several times at various surgical conventions in the United States. He never forgot to ask me whether I had learned meanwhile about Jesus and what I think about him now. Both Dr. Neely and Dr. Wofford had been Dr. Hardy’s residents some years earlier. Both were excellent surgeons and teachers and I learned a lot from them. The third surgeon, Dr. Hans Karl Stauss, a German, was born in Dresden in eastern Germany and spent a major part of his life in Romania. He arrived in the United States after World War II and settled in Mississippi. He was friendly toward me and showed great interest in my past in Europe. Dr. Stauss was a good teacher, but as a surgeon, did not equal his two friends. During my six-month rotation at the Sanatorium, I performed under the guidance of these three surgeons 77 thoracic operations. This included pneumonectomies, lobectomies, thoracoplasties of every possible kind and others. As far as operative and clinical experience is concerned, my work at this hospital for tuberculosis was for me the richest and most rewarding period ever.
Wednesdays at the Sanatorium were devoted to bronchoscopies 7 and bronchographies 8. These procedures were performed on the conveyor belt principle: nurses placed the first patient on the table and started applying local anesthetic to the larynx. I continued with the anesthesia (always local), performed bronchoscopy, and concluded the procedure by injecting contrast medium through a fine catheter into the bronchi. While I was recording the bronchoscopy findings, the nurses took the patient to the Radiology Department for a series of roentgenograms taken at various angles. Meanwhile, I started working on the next patient. At the end of the day’s work, I saw and interpreted all the roentgenograms and compared them with the bronchoscopy findings, as recorded earlier. On an average day there were between 10 and 20 bronchoscopies and bronchographies. All this was done without the help of an anesthesiologist or a radiologist, as such specialists were not on the Sanatorium staff. The work was completed by midday. Then I collected all the roentgenograms and drove to the University Hospital in Jackson – a trip of over one hour – for a conference with my three instructors. They praised my work and decided on further treatment of the patients. The majority were operated on during the following week. In the middle of the conference there was a coffee break (actually, this was my Wednesday lunch). We discussed the white patients before the break and the black ones after (Fig. 18). An important detail should be pointed out: this
separation by race was exercised only with regard to patients from the Sanatorium. At the University Hospital and the Veterans Administration Hospital the conferences were integrated with no regard to skin color. Racial separation was abolished in the mid-1960s in all hospitals and other institutions that received financial support from the federal government. This change occurred in all Veterans Administration hospitals in the United States, and also in “our” University Hospital, but not in the Mississippi State Sanatorium, which was financed entirely by the government of the State of Mississippi. Accordingly, the segregation at the Sanatorium remained in power, and was not limited to conferences. The institution was based in two buildings: the “Sanatorium”, where white patients were hospitalized (Fig. 19), and the “Colored Infirmary” for blacks (Fig. 18). Each of the buildings had separate teams of nurses and other employees (it was inconceivable that a white nurse would serve black patients), although there was only one team of physicians – all white.
A typical characteristic of Southerners is considerable politeness and notable formality. Except for relatives and close friends, one never addresses people by the first name, only as Mr. or Ms. with the surname following. In my “ignorance”, I used this formal approach with regard to everybody, including my black patients. This resulted occasionally in a misunderstanding, because the blacks did not understand that I was talking to them, and did not respond. However, a corrective remark by one of the nurses was not late to come: “Doctor, we do not call them Mr. or Ms. Her name is Jessie.”
The struggle of blacks for equality in the Southern States reached its peak while I was there. In the summer of 1966 I happened to witness a demonstration in Jackson. Two competing groups of demonstrators arrived in town. One was headed by Martin Luther King, Jr., the other by one of the more violent activists; if my memory does not fail me, it was Stokely Carmichael. Both groups met in one of the town’s main squares. The two groups stood opposite each other. The Carmichael group shouted in unison “power!”, and the group led by King, responded “freedom!”, and so alternating: “power - freedom - power - freedom”. Blood was not spilled. I may have felt lonely in Mississippi, but there was no boredom.
While working at the Sanatorium, I lived in a comfortable house, sufficient for a whole family. Many of the employees lived on the hospital grounds, in similar houses. During a tornado that struck Mississippi (the only one that I have experienced in reality, not on television), I locked myself in the house and worried that the wind might blow it away along with me, as happened to quite a few uprooted trees and some cars. But my house was strong enough and remained firmly on the ground. My Volkswagen, likewise, did not suffer any damage (Fig. 20).

I had good and friendly neighbors who made every attempt to help me, according to their best understanding. For example, my secretary, Mrs. Mary Polk – like Dr. Wofford, religious to the extreme – overwhelmed me with invitations to visit her church and meet her pastor. Later she implored that I tell them about “the land where Jesus walked”. After several such requests, I accepted the invitation and took my slides and projector to their church. My slide show must have disappointed them, at least to some extent, because presumably they expected to hear about the primitive life in the Holy Land: shepherds and sheep – as in the days of Jesus; also, they probably expected me to tell them more about the Christian holy places and about Jesus himself. Views of contemporary Jerusalem and Tel Aviv, the Hadassah Medical Center (less impressive than the buildings of the University Hospital in Jackson), and sunbathing beauties at the seashore in Haifa were not of particular interest to them. Despite that, Mrs. Polk continued with invitations to visit her church, but I became more resistant and did not come again. Mrs. Polk remained a good and faithful secretary, and her husband, the best barber in Magee, cut my hair every month with great expertise.
* * *
The news about the Six-Day-War reached me in the most peculiar way. For a long time before the war started, television and radio programs abounded in threats by Arab leaders who predicted prompt destruction and elimination of the State of Israel. They were arrogant and brazenly self-confident. The economic stagnation in Israel reached new depths. It seemed, that in a well coordinated war effort against Israel, the Arab armies might overcome Israel and materialize their threat. The situation was very grave and there was a general feeling of an approaching war.
On June 5th 1967, while I was on the rotation at the Sanatorium, I woke up later than usual and, contrary to my routine, did not have time to listen to the radio newscast. Without knowledge of the last 24-hour developments in Israel, I went to the operating room. I had just completed a bronchoscopy, when one of the nurses called me to the telephone. It was from the Israeli consulate in New York. They told me that the war had just begun, there is an urgent need for Doctors, and asked me to fly to Israel as soon as I can.
I left the operating room, drove to Jackson, entered Dr. Hardy’s office and told him that I must leave for Israel immediately (Fig. 21). At the Kennedy Airport in New York, an immense crowd of Israelis was waiting for flights to Israel. But the number of planes and flights was limited, and the chances to fly “immediately” were slim. Everybody had good reasons to get to Israel, and my argument that I am a surgeon, did not impress the El Al clerks very much. I waited in the airport on a stand-by basis for a couple of days, with minimal hope and no result. In the meantime, the political and military situation in Israel changed completely. Israel prevailed on all fronts and won the war. I returned to Mississippi to continue my work.
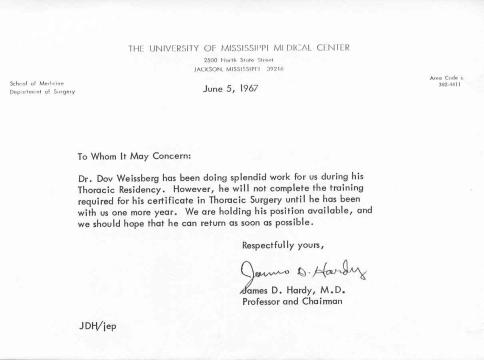
Fig. 21. The Six-Day-War letter from Dr. Hardy, June 5th 1967.
* * *
I heard about mediastinoscopy for the first time at the congress of the American Association for Thoracic Surgery in Montreal, in the spring of 1964. Dr. State, always utterly concerned about the education of his residents, used to send us to scientific conventions. He knew about my interest in thoracic surgery and decided that I should go to Montreal. One presentation at the convention arose my particular interest: it was a report on mediastinoscopy with experience in 74 patients. The material was presented by a young surgeon from Toronto, Dr. Frederick Griffith Pearson.
Mediastinoscopy, a method of exploration of the mediastinum 9, is indicated in patients with enlarged lymph nodes or other masses in this anatomic area. The procedure consists of a direct inspection of the mediastinal contents and obtaining tissue sections for microscopic examination. It is particularly important in patients with lung cancer. The spread of cancerous cells from the primary lung tumor to the mediastinum is a contraindication to major lung surgery, and a documentation of such metastatic spread has important therapeutic implications. I was greatly impressed by the usefulness of this procedure and easiness of its performance. The clarity of the presentation enhanced my interest in the subject. I became obsessed with the idea of mediastinoscopy, and upon my return to New York, suggested to the chief of the thoracic surgery service, Dr. Robert Frater, that we introduce it to our clinical practice. However, Dr. Frater thought that the procedure was hazardous and expressed objections. He also thought that any new method, such as mediastinoscopy, should be concentrated initially in the hands of only one person, who would first learn it well and then teach others. At that time I was the only one in the hospital with an interest in mediastinoscopy and spent only short rotations on the thoracic service. It was not possible for me to take charge of this new operation. Thus my pleas to Dr. Frater did not lead to any results. But the idea remained in my head.
After several months in Mississippi I suggested to Dr. Hardy, as to Frater before him, that we start doing mediastinoscopies. Dr. Hardy, likewise, did not become excited with the idea. He pointed out the dangers. Mediastinum contains large blood vessels, heart and other organs. The method of inspecting mediastinum is performed through a 25 mm incision in the neck. Through this incision the operator inserts the scope – a metal tube illuminated at the end. The area of inspection is limited by the 15-mm internal diameter of the scope. During the procedure blood vessels might be injured, with possible life-threatening bleeding. Still, I was not ready to give up, and waited for a suitable case. A short time later, a patient with lung cancer was admitted to our service. Roentgenograms showed enlarged lymph nodes in the mediastinum, and metastatic spread was suspected. When Dr. Hardy repeated his warnings about the possibility of complications, I said: “Dr. Hardy, you were the first surgeon to perform human lung and heart transplantations; you are doing kidney transplantations and open heart operations; are these not dangerous procedures? What about medical progress?”. Hardy thought for a moment and said: “Well, try, but be careful!” The next day I performed the first mediastinoscopy in Mississippi. I had no previous experience with it, and felt a burden of great responsibility and fear of complications. I knew that I must not fail, and worked with extreme caution. Thus my first exploration of the mediastinum was very limited; as a matter of fact, it was incomplete. Yet, I was very lucky, and this limited procedure sufficed: next to the windpipe I felt a firm nodule – an abnormal finding in any mediastinum. I took a small section of the nodule for biopsy and did not look for more. Histologic examination of the tissue disclosed a metastasis of lung cancer. The importance of this finding could not be overrated. It prevented a major operation: an unnecessary thoracotomy. Dr. Hardy felt that progress has been made. He smiled and summarized the subject in one sentence: “Dov, you have my permission to do mediastinoscopies”. So I did. The results were not always as clear-cut as on the first case, but I always managed to avoid complications. The feeling of great satisfaction that I was the first surgeon to perform mediastinoscopy in Mississippi (and later in Israel as well) has not left me until this very day. For historical honesty, I must admit that I learned the proper technique of mediastinoscopy later, while working on the service of Dr. Pearson in Toronto, the same surgeon who summarized his experience with mediastinoscopy at the convention in Montreal.
* * *
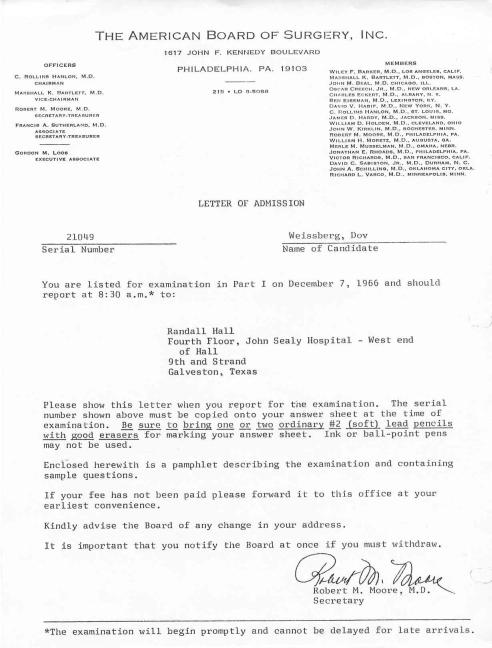
To complete the process of obtaining a specialist certificate, one must pass the examination of the American Board of Surgery. The examination is composed of two parts. Part I is a written examination and includes, in addition to surgery, also basic sciences. Only the candidates who pass this part, can apply for Part II – the oral examination. After completing my residency in June, the earliest date of the written examination, was December 7th 1966. On this day the examination was held in several cities; the nearest to Mississippi was Galveston, Texas (Fig. 22). I used part of my annual vacation, and after the examination stayed in Galveston a day longer, to see this historically interesting city. From there I went to the National Aeronautics and Space Administration (NASA) and to the Baylor University Medical Center in Houston. I managed to have a look at the superstars of cardiovascular surgery in America – Drs. DeBakey, Cooley and others of worldwide fame.
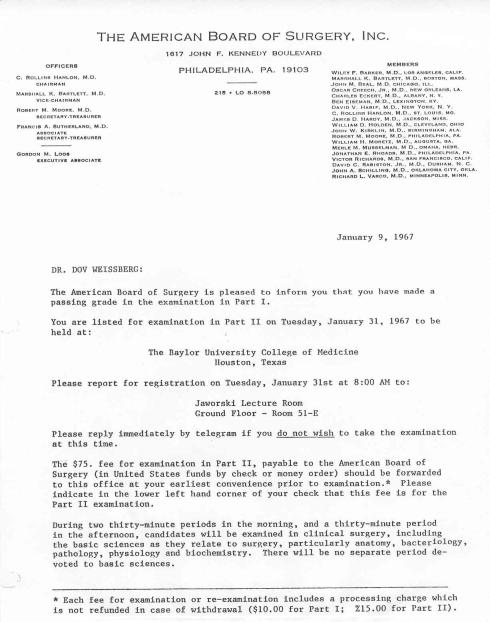
The oral examination took place in Houston on January 31st 1967 (Fig. 23). The atmosphere was relaxed. Dr. DeBakey, usually feared by those he examined, was among my examiners, but was simply charming (Fig. 24). After the examination I stayed in Houston for ten days, again to see the “superstars” operating. The volume of their work, their organization and efficiency were exemplary and exceeded all that I had expected or could have imagined. Between operations, Dr. Denton Cooley invited me for a short conversation over a cup of coffee.
I received my specialist certificate after several weeks (Fig. 25).
As in general surgery, the examination in thoracic surgery could also be taken only after completing the residency. However, my visit in the United States as a trainee in surgery was initially limited to five years. For the purpose of residency in thoracic surgery my stay was extended for an additional two-year period, but this extension was final, with no possibility of appeal. I could not stay in the United States beyond June 30th 1968.
In order to enable me to take the examination and obtain specialist certificate, Dr. Hardy used his influence with the American Board of Surgery, and I was given permission to be examined while still in training. The examination dates given to me were April 20th and 21st 1968. The examination took place in Pittsburgh, during the days preceding a convention of thoracic surgeons in that city (Figs. 26 and 27). This examination, likewise, was successful (Figs. 28-30).
Fig. 26. Admission letter for examination in thoracic surgery.
Fig. 27. Examination card of candidate No. 75.
Fig. 28. Letter informing me of examination results.
Fig. 29. Specialist certificate in thoracic surgery.
Fig. 30. Congratulatory letter from Dr. David State.
* * *
Equipped with specialist certificates in general and in thoracic surgery, I was ready to return to Israel, and I hoped that this would become possible as soon as my residency was completed. But it was not a simple matter. Before I left Israel, Dr. Prywes from the medical school told me that every physician who succeeds in training in America, returns to Israel with demands that the Israeli hospitals, as a rule, cannot accept. The return to Israel is thus delayed, and, eventually, the successful graduate stays in America permanently. Professor Rachmilevitz, likewise, was let down by my decision to seek training abroad, and accused me of abandoning Israel. At that time I did not believe that this could happen to me, but now his prophesy threatened me.
As early as during my work in the Rambam Hospital, I felt the heavy hand of my seniors. I dreamed that some time in the future, I would become chief of my own service. During the two years spent in Dr. Hardy’s department, this feeling consolidated. Hardy was a great teacher and represented the best in medical education and in surgical progress, but during all the time spent under him, I felt like a slave. More than anything, I wanted to obtain a position of department chief. No more serving another master. Assuming that I would start working in Israel in someone else’s department, it was very unlikely that the chief would be to my taste. Much more likely he would be similar to Jack Abouav’s boss at the Rambam Hospital. This possibility was unacceptable to me. I felt that my knowledge and experience were sufficient for heading a department of my own. During my visit in Israel in 1965 I met several high-ranking personalities in the Ministry of Health, the central offices of Kupath Holim (health services of the Labor Federation) and other institutions. I told them about my plans to return to Israel, and about my expectations. They were ready to offer me a job in almost every hospital, but no one offered me a service of my own. As a matter of fact, I was not surprised. They did not know me and had not seen me working. The risk of accepting a “stranger” for a position of chief was too great.
Following my visit in Israel, I continued to correspond with people who could offer me a job, but I received only hints and implications as to the future. These did not satisfy me.
Because I had to leave the United States by June 30th, it seemed that the best solution for me would be accepting a temporary job in Canada. I had no desire to stay in Canada permanently, but while working in Canada, I would continue maintaining contacts with medical institutions in Israel.
I initiated contacts with several medical centers in Canada. The most attractive response came from Dr. William Drucker, Chairman of the Department of Surgery at the University of Toronto. Dr. Drucker informed me about his plans to establish a general thoracic surgical division, separate from heart surgery. In view of my qualifications, he was willing to consider accepting me to the staff of the new division. He invited me for an interview.
In Toronto, in addition to Dr. Drucker, I met the appointed chief of the soon-to-be-opened new division – Dr. F.G. Pearson, who interviewed me, showed me the hospital and invited me to the operating suite to see some of the operations scheduled for that day. The first procedure on the schedule was mediastinoscopy. At this point I suddenly realized that Dr. Pearson is the same one who lectured on mediastinoscopy in Montreal in 1964. At the end of the interview I was accepted to the new division as a senior fellow in thoracic surgery for one year, with a possibility of an extension for another year.
7 Direct observation of the bronchi through the bronchoscope.
8 Roentgenography of the bronchi with the use of contrast medium.
9 Mediastinum is the central area of the chest, located between the two lungs.